When the Lining Was Never the Same
An expanded analysis of AGCES 2026, integrating emerging clinical frameworks in Adenomyosis and Endometriosis

Endometriosis and adenomyosis are not simply bad periods. They are chronic diseases. They cause real pain, real disability, and real life disruption.
For thousands of years, severe pelvic pain was brushed off as something women were supposed to endure. Mothers told daughters it was normal — teachers said it was part of growing up. Even doctors were trained to believe it was just how female bodies worked. But what if the lining was never the same to begin with?
Inside the uterus is a layer called the endometrium. This lining thickens each month. If pregnancy does not happen, it sheds. That shedding is a “period”. It is predictable. It responds to hormones in a pattern.
That is normal endometrium. Now for the mind blowing part. Endometriosis is not that, and we are seeing new things with adenomyosis too.
Generations upon generations were told endometriosis was just bits of that lining that traveled backward during menstruation and implanted in the pelvis. That theory shaped medicine for over a century. It sounded simple — it was easy to repeat.
But it never explained everything. It did not explain why endometriosis has been found in young girls before their first period, in fetuses animals or even cases of cis men. It did not explain why lesions show up on the bowel, the diaphragm, or wrapped around nerves. It did not explain why the tissue behaves differently at a biological level.
Endometriosis lesions are not misplaced lining. They are abnormal cells that create lesions that produce their own estrogen. They often resist progesterone. They trigger ongoing inflammation. They grow new nerve fibers. They create pain that does not follow the rhythm of an external cycle — while self stimulating it’s own internal process.
They do not shed and disappear each month. Much of the misunderstanding around endometriosis comes from the idea that it behaves like that normal endometrium but outside the uterus. That it sheds, bleeds, and somehow redistributes through processes like retrograde menstruation. But that is not what we are seeing.
Endometriotic lesions are not simply pieces of lining that detach and relocate. They are biologically active tissue — they grow, invade, and sustain themselves in ways that normal endometrium does not. While bleeding can occur within or around these lesions, it is not the result of a coordinated shedding process. It is more often tied to inflammation, vascular changes, organ/tissue damage and the fragile, reactive nature of the tissue itself.
In some cases, lesions can appear blister-like, cystic, or deeply infiltrative. They can be clear, red, black, or fibrotic. They may spread across surfaces, wrap around structures, or burrow into tissue. These variations are not cosmetic differences. They reflect different biological behaviors.
What may look, at a glance, like “internal bleeding from a period” is not the same process at all. That misunderstanding has shaped decades of oversimplified explanations. That is why calling endometriosis a painful period is not just inaccurate — it is harmful.
Adenomyosis is also different in it’s own way, but it has been tangled into the same confusion. Adenomyosis happens when tissue similar to the inner lining grows into the muscle wall of the uterus. The muscle becomes thick and inflamed. The uterus can enlarge. Bleeding can become heavy. Cramps can become unbearable.
Under a microscope, adenomyosis and endometriosis can both show certain glands and supportive tissue called stroma. Normal endometrium also has glands and stroma. That overlap shaped decades of thinking.
But similar does not mean identical. More importantly, that was never the full picture.


More Than Glands and Stroma
For years, these glands and stroma were treated as the defining features of these diseases. They became the main course of how we understood them. Everything else was secondary or even non-existent. We are now beginning to understand that those features were only the starting point.
Beyond those structures is an entire biological environment that changes how both of these diseases behave — hormone signaling shifts, local estrogen production increases, progesterone resistance develops. The immune system responds differently. Inflammation becomes chronic. Nerve fibers grow where they should not and blood vessels reorganize. The tissue remodels itself. These are not supporting details — they are what define the disease itself.
Adenomyosis, in particular, reshapes the muscle of the uterus. The myometrium becomes reactive — it thickens. It changes how the uterus contracts and how blood flows through it. That environment is not passive. It is active and constantly influencing what happens inside the uterus.
Endometriosis behaves differently. It survives outside the uterus in environments where just don’t make sense. It sustains itself. It signals independently. It interacts with surrounding organs, nerves, and immune pathways in ways that normal endometrium does not.
So while these conditions may look similar in structure, they begin to separate in behavior. When we build entire frameworks of care based on what looks similar under a microscope, we risk missing everything happening beyond it.
For years, we focused on what was visible and overlooked the rest of the system. But the rest of the system is where the impact sits.
Why We Confused Them in the First Place
The confusion around these diseases was not random. It was built into how they were defined.
When the defining features are reduced to those microscopic glands and stroma, it becomes easy to group conditions together. It becomes easy to assume they share the same origin. It becomes easy to treat them as variations of the same process. That assumption shaped everything that followed and has been where we sat for quit literally 100 years — stand still research, diagnostics, and treatment. It delayed deeper understanding.
Adenomyosis could only be definitively diagnosed after hysterectomy for most of it’s time. That meant most research came from later-stage disease. We were studying what the condition looked like at the end, not how it developed over time. Now, with advances in imaging and emerging approaches to tissue sampling, we are beginning to see these diseases earlier and more clearly.
That shift is significant here. When we can study disease before organ removal, we can begin to understand its progression — not just its outcome. It also forces us to re-examine treatments built on incomplete understanding.
Procedures like uterine ablation target the inner lining of the uterus — but adenomyosis exists within the muscle. Treating the surface does not resolve what lies beneath it. In some cases, it can complicate diagnosis or leave the underlying disease unchanged. Same goes for ablation of endometriosis outside of the uterus.
When we only treat what is visible, we risk missing what is driving the condition. Better tools bring better clarity, clarity changes care.
Even the Definition Isn’t Settled
What becomes clear in current research is that the confusion is not just historically ongoing. There is still no universally accepted classification system for adenomyosis alone — not in imaging, not in pathology, not in how severity or subtypes are defined. Classification is not just academic. It determines how disease is recognized, how it is studied, and how treatment decisions are made.
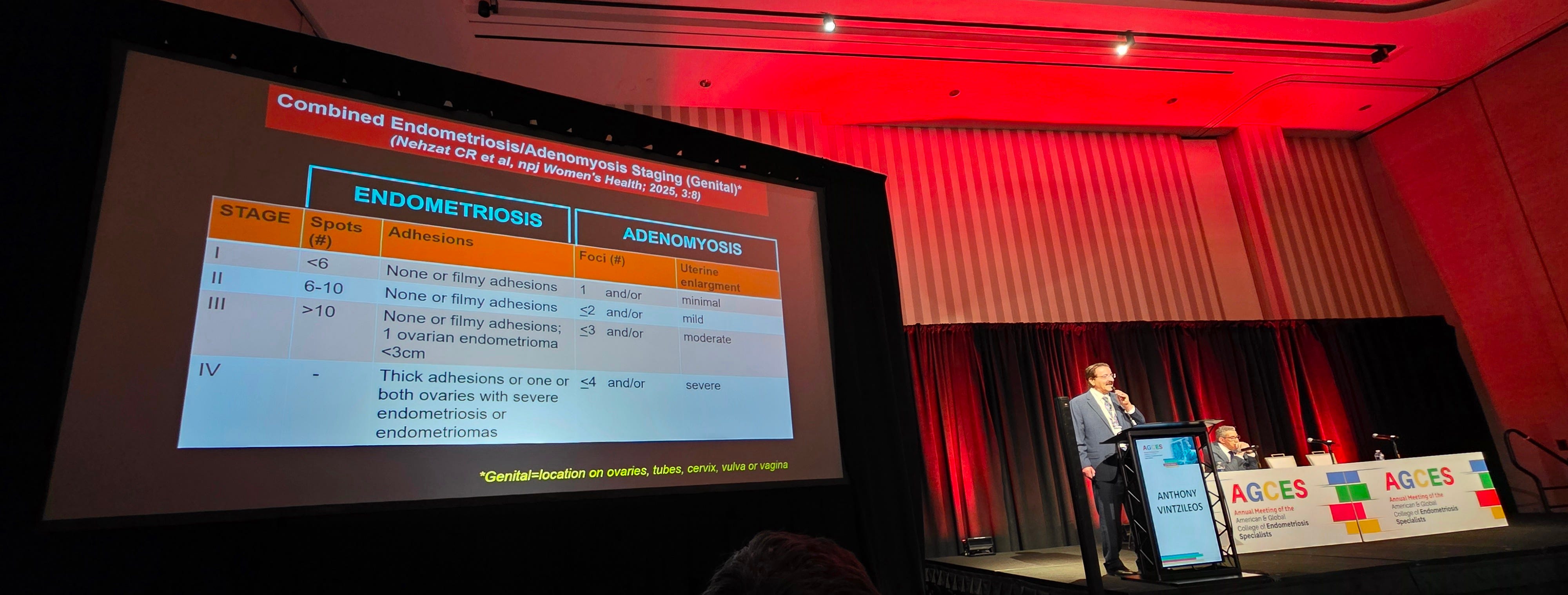
This is part of why newer frameworks are beginning to shift the conversation. The AGE Classification System proposes separating adenomyosis, genital endometriosis, and extragenital disease into distinct but connected components, emphasizing anatomical involvement, disease burden, and surgical complexity. Rather than forcing these conditions into a single simplified category, it reflects something patients have long experienced — that these diseases do not follow one pattern. When classification begins to match biological reality, it changes how we stage disease, how we plan treatment, and how we measure outcomes.
Only more recently have imaging tools like ultrasound and MRI allowed clinicians to identify adenomyosis without removing the uterus. That shift has expanded visibility, but it has also exposed variability. Not just in how the disease presents, but in how it is interpreted. There is also no single agreed standard for how adenomyosis should appear on imaging either. Findings overlap. Criteria differ. What one provider identifies, another may miss.
What is seen does not always match what is felt — some patients with extensive disease may have minimal symptoms. Others with less visible findings experience severe pain, bleeding, and disruption to daily life. That disconnect reflects something patients have been saying for decades. Severity cannot be measured by appearance alone.
There are also emerging distinctions within adenomyosis itself. Some researchers describe internal forms affecting the inner uterine layers, and external forms located closer to the outer wall, sometimes overlapping with endometriosis. This is not just structural. It raises deeper questions about how these diseases overlap and how they are treated.
Even here, the origin is debated. Does the disease begin within the uterus and move outward overtime? Does it arise from processes outside the uterus and move inward, blurring the boundary even more? These are not minor differences in theory. They shape how we interpret imaging, how we classify disease and how we approach treatment. If internal and external forms develop through different mechanisms, then grouping them under a single label may overlook important biological differences.
This may also may help explain why some patients present with overlapping features of both conditions, and why separating them clinically is not always straight forward. What appears as two diagnoses may — in some cases — reflect a shared or interacting processes. But processes that differ from the native endometrium.
The answer is not settled. That uncertainty is not weakness in the field, just a signal that we are finally asking more precise questions. We are not working from finished definitions. We are working from moving ones and only now beginning to build systems capable of keeping up.
Which means the patients who have lived with this disease were never the outliers, they were the evidence. This is where the distinction stops being theoretical — because when we misunderstand what these diseases are, we misunderstand what they are doing inside the body.
Nowhere is that disconnect more consequential for many, than in pregnancy, fertility, and early development.
Pregnancy, Fertility, and Fetal Development
One of the more grounding realities is how these diseases influence pregnancy, fertility, and early development.
Adenomyosis directly alters the uterine environment. It changes the structure of the muscle, the way the uterus contracts, and the vascular system that supports implantation. Chronic inflammation and immune changes can make implantation more difficult and influence pregnancy as it progresses.


This is reflected in increased risks of preterm birth, placental abnormalities, hypertensive disorders, and postpartum hemorrhage. Adenomyosis does not pause during pregnancy — it continues to shape the environment in which that pregnancy develops.
Endometriosis often impacts the process even earlier. It contributes to infertility through inflammation, anatomical distortion, and hormonal disruption. Even with assisted reproductive technologies, outcomes can be more complex.
When both conditions are present, those effects can compound. The focus cannot stop at whether pregnancy is possible. It has to include what happens after.
For years, these diseases were framed through reproduction alone. Pain was secondary. Immune dysfunction was barely studied. Pregnancy outcomes or complications never truly acknowledged. Research involving women was not consistently required until the 1990s — but things are slowly changing as move through the years.
Endometriosis and adenomyosis are now being recognized as complex, systemic, inflammatory diseases. We are not looking back at that shift. We are living in it daily. The last thirty years have brought more progress to women’s health than the centuries before them.
This does not end here — what we understand today is not final. It is a foundation. These outcomes are not separate from the disease itself. They are simply the disease being ignored and reduced. We have misunderstood these diseases because the system has insisted they were simple.
Where the Lines Begin to Blur
There is no cure for endometriosis. A hysterectomy, however, is a cure for adenomyosis since it is contained to the uterus. Treatments exist, but they are not perfect for either.
These diseases are complicated, and they are very real. I know this not just from research, but from my own life. As a teenager, I was told my pain was hysteria. Years later, after severe complications and multiple surgeries, I learned I had both endometriosis and adenomyosis — my uterus was removed.
The pain did not disappear all together. Some symptoms improved without the influence of what adenomyosis was doing alongside the endometriosis and other inflammatory triggers in my body.
When we finally separate normal tissue from disease, we begin to see it clearly. Endometriosis and adenomyosis are not weakness or basic women processes. They are chronic inflammatory diseases that deserve modern science, accurate definitions, and earlier recognition.
Pain that disables people is not normal, for anyone. The reality is finally being acknowledged and frameworks are shifting. The lining was never the same and neither was the disease.